Elvis was a 5 yr MN Great Dane who presented to our surgery service for a mass at the level of the right caudal chest. His owners reported that they first noticed the mass about three months ago and it had been rapidly growing since then. Besides the mass he appeared comfortable and was otherwise eating and drinking well.
Dr. Marta Agrodnia performed a thoracic CT which revealed a large contrast enhancing mass along the right rib cage, with growth into the thoracic space. A surgical biopsy was obtained under general anesthesia, which returned as favoring a chondrosarcoma. The pathologist noted 4 mitoses in 10 high power fields (MI = 4). There was no vascular invasion noted throughout the biopsy and the pathologist suggested the microscopic features were most suggestive of a grade I chondrosarcoma.
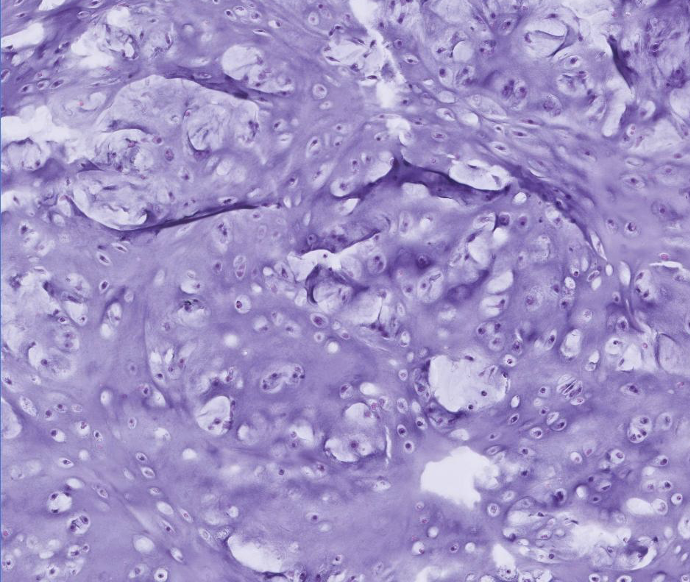
Elvis’s surgical biopsy following thoracic CT: The poorly demarcated and highly cellular mass is composed of polygonal cells embedded in lacunae which are separated by abundant chondroid matrix. Multifocally, there are 2-4 cells per lacunae with neoplastic cells having moderate nuclear pleomorphism.
Surgical resection was recommended due to the invasive nature of the mass and increased survival time associated with tumor excision. Due to the rapid rate of growth it was discussed with his owners that there was a risk of a more guarded prognosis, if excisional biopsy revealed evidence of osteosarcoma.
Both mass removal and rib resection were performed by Dr. Agrodnia (pictures included at the bottom of this article):
- Preoperative ultrasound-guided intercostal blocks were performed by Dr. Raphael Vizena using ropivacaine
- An elliptical incision was made over the right caudal thorax. Hemostasis was managed with both electrocautery and Ligasure.
- All visually abnormal tissue was removed, along with 2-4 cm margins on all normal appearing fat and muscle.
- A sagittal saw was used for resection of ribs 8, 9, 10, and 11
- The diaphragm was reattached to the body wall using interrupted cruciate sutures
- Two pieces of SurgiMesh (15 x 7.5 cm) were placed in the chest wall defect and then secured into place with interrupted cruciate sutures, taking care to keep the knots external to the mesh and buried into tissue.
- The two mesh pieces were also secured together, and a chest tube was placed under mesh.
- Closure was performed in two layers and Nocita was placed locally
- A trans-costal epidural soaker catheter was placed as well as a sterile bandage.
Elvis recovered uneventfully from surgery. The mass Dr. Agrodnia excised weighed 3.06 kg, and histopathology confirmed the diagnosis of a chondrosarcoma. As of the date of this publication, Elvis has had no recurrence of his rib mass. He met with our oncology service to initiate metronomic chemotherapy (chlorambucil) shortly following surgery, to decrease the risk of tumor regrowth.
CLINICALLY RELEVANT FACTS:
- Chondrosarcoma is the second most common primary bone neoplasia in canines. Dogs who are medium to large breed, and middle age to older are predisposed. These tumors arise from cartilage and tend to involve flat bones (ribs, turbinates, pelvis, etc). They are considered malignant tumors, however they often have a low metastatic rate with some data suggesting a rate of 20% or lower.
- Surgical excision is recommended to decrease the risk of metastasis, and therefore prognosis has historically been linked with anatomical location (depending on the potential for complete excision). Local invasion and recurrence can occur after surgery, so owners should be warned of these risks.
- The major differential for chondrosarcoma includes osteosarcoma, which carries a much higher metastatic rate and guarded prognosis. Caution should be used when discussing prognosis and making a treatment plan in cases like Elvis, where a small surgical biopsy (in comparison to the entire 3.06 kg tumor) is used to diagnose the tumor type. Luckily Elvis’ surgical excision confirmed chondrosarcoma, however surgical biopsy in similar cases may underestimate the grade or misdiagnose the tumor type depending on which part of the mass was sampled. If excisional biopsy was suggestive of osteosarcoma, a more guarded prognosis for metastasis would have been reported to the owner. This would also impact how the PVESC oncology service would manage his case.

The red circle outlines the border of the right rib mass, visible just prior to surgery. This mass had been visible to the owners for about 3 months and they felt it was rapidly growing and non-painful. The previous incisional biopsy site (post thoracic CT) is visible.

Dr. Agrodnia has the large tumor in her arms (the tumor can be seen labeled by the yellow arrow), carefully removing the last few connections between the tumor and Elvis’ body.
The tumor weighed 3.06 kg upon removal.

Both pieces of mesh are sutured into the chest wall defect (white arrows), and to each other (purple arrow). The chest tube can be seen below the mesh.
Authored by: Dr. Landry, DVM, DACVIM, Neurology